If you appreciate this website, please help us maintain and update the Micronutrient Information Center. Make a gift during Oregon State University's annual giving drive.
April 24 is Dam Proud Day, our annual day of giving. Support the Linus Pauling Institute with a donation on this day and help us unlock over $60,000 of challenge gifts!
Learn more on our Dam Proud Day website
Contents
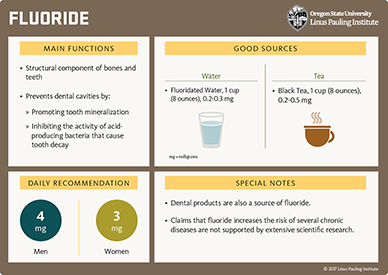
Fluorine occurs naturally as the negatively charged ion, fluoride (F-). Fluoride is considered a trace element because only small amounts are present in the body (about 2.6 grams in adults), and because the daily requirement for maintaining dental health is only a few milligrams a day. About 95% of the total body fluoride is found in bones and teeth (1). Although its role in the prevention of dental caries (tooth decay) is well established, fluoride is not generally considered an essential mineral element because humans do not require it for growth or to sustain life (2). However, if one considers the prevention of chronic disease (dental caries) an important criterion in determining essentiality, then fluoride might well be considered an essential trace element (3).
Fluoride is absorbed in the stomach and small intestine. Once in the bloodstream it rapidly enters mineralized tissue (bones and developing teeth). At usual intake levels, fluoride does not accumulate in soft tissue. The predominant mineral elements in bone are crystals of calcium and phosphate, known as hydroxyapatite crystals. Fluoride's high chemical reactivity and small radius allow it to either displace the larger hydroxyl (-OH) ion in the hydroxyapatite crystal, forming fluoroapatite, or to increase crystal density by entering spaces within the hydroxyapatite crystal. Fluoroapatite hardens tooth enamel and stabilizes bone mineral (4).
Both calcium and magnesium form insoluble complexes with fluoride and are capable of significantly decreasing fluoride absorption when present in the same meal. However, the absorption of fluoride in the form of monofluorophosphate (unlike sodium fluoride) is unaffected by calcium. Also, a diet low in chloride (salt) has been found to increase fluoride retention by reducing urinary excretion of fluoride (1).
In humans, the only clear effect of inadequate fluoride intake is an increased risk of dental caries (tooth decay) for individuals of all ages. Epidemiological investigations of patterns of water consumption and the prevalence of dental caries across various US regions with different water fluoride concentrations led to the development of a recommended optimum range of fluoride concentration of 0.7-1.2 milligrams/liter (mg/L) or parts per million (ppm); the lower concentration was recommended for warmer climates where water consumption is higher, and the higher concentration was recommended for colder climates. In 2015, the US Department of Health and Human Services recommended that all community water systems adjust the fluoride concentration to 0.7 mg/L, as more recent studies did find a relationship between water intake and outdoor air temperature. This recommendation was made in an effort to reduce the risk of dental fluorosis (see below) and in light of the widespread availability of fluoride from other sources, including fluoride-containing oral-care products (5). A number of studies conducted prior to the introduction of fluoride-containing toothpastes demonstrated that the prevalence of dental caries was 40% to 60% lower in communities with optimal water fluoride concentrations than in communities with low water fluoride concentrations (6).
The Food and Nutrition Board (FNB) of the US Institute of Medicine updated its recommendations for fluoride intake in 1997. Because data were insufficient to establish a Recommended Dietary Allowance (RDA), Adequate Intake (AI) levels were set based on estimated intakes that have been shown to reduce the occurrence of dental caries most effectively without causing the unwanted side effect of tooth enamel mottling known as dental fluorosis (0.05 mg/kg of body weight) (Table 1; 6). See the section below on Safety for a discussion of dental fluorosis.
Specific cariogenic (cavity-causing) bacteria (mainly Streptococcus mutans and Streptococcus sobrinus) found in dental plaque are capable of metabolizing fermentable carbohydrates (sugars) and converting them to organic acids that can dissolve sensitive tooth enamel. If unchecked, the bacteria may penetrate deeper layers of the tooth and progress into the soft pulp tissue at the center. Untreated caries can lead to severe pain, local infection, tooth loss or extraction, nutritional problems, and serious systemic infections in susceptible individuals (7). Dental caries — both treated and untreated — contribute to diminished overall oral health, which, in turn, may affect systemic health. For example, some observational studies have suggested a link between systemic inflammation in individuals with periodontal (gum) infection and insulin resistance (8), type 2 diabetes mellitus (9), hypertension (10), and coronary heart disease (11). Moreover, the bacterium causing periodontitis, Porphyromonas gingivalis, may be linked to rheumatoid arthritis (12, 13). Poor oral health in general may constitute a risk factor for coronary heart disease (14) and other cardiovascular diseases (15, 16).
Increased fluoride exposure, most commonly through community water fluoridation, has been found to decrease the incidence of dental caries in children and adults (17, 18). Between 1976 and 1987, clinical studies in several countries demonstrated that the addition of fluoride to community water supplies (0.7-1.2 ppm) reduced caries by 30%-60% in primary (baby) teeth and 15%-35% in permanent teeth (19). A 2015 review and meta-analysis of prospective observational studies found a 35% and 26% reduction in number of decayed, missing, and filled primary and permanent teeth with consumption of fluoridated versus non-fluoridated water, respectively (20). While fluoride’s prevention of dental caries is primarily through topical action, fluoride consumed in water appears to have a systemic effect in children before all teeth have erupted — typically through 12 years of age.
Fluoride is incorporated into the developing enamel of teeth and increases the resistance to caries. Since the caries preventative effect of fluoride is also topical (surface) in children after teeth have erupted and in adults, the optimal protection achieved by fluoridated water likely occurs through both systemic exposure before and after tooth eruption and topical exposure after tooth eruption.
Research has indicated that the primary action of fluoride occurs topically after the teeth erupt into the mouth. Ingested fluoride is secreted in the saliva and contributes to topical protection. When enamel is partially demineralized by organic acids, fluoride in the saliva can enhance the remineralization of enamel through its interactions with calcium and phosphate. Fluoride containing remineralized enamel is more resistant to acid attack and demineralization. In salivary concentrations associated with optimum fluoride intake, fluoride has been found to inhibit bacterial enzymes, resulting in reduced acid production by cariogenic bacteria (7, 17).
The use of topically applied fluoride-containing products, including toothpaste, gel, varnish, and mouth rinse, is thought to have contributed to the substantial decrease in the prevalence of caries over the last decades (21). A 2013 meta-analysis of fluoride interventions in children and adolescents (up to 16 years of age) found that the application of fluoride varnish for at least one year was associated with a 37% reduction in decayed, missing, and filled tooth surfaces in decayed tooth surfaces of primary teeth; the anti-caries effect on the permanent teeth corresponded to a 43% decrease compared to no treatment or placebo (22). A recent (2021) meta-analysis of topical fluoride reviewed 15 clinical trials with 9,541 participants. Specifically, the meta-analysis evaluated 14 trials of fluoride varnish compared to placebo or no fluoride and one trial of fluoride foam, and found that topical fluoride reduced dental caries increment by about one tooth surface over a two-year period (23). The same meta-analysis also found that fluoride varnish significantly prevented any incident dental caries, but only for children who were younger than 2 years of age (23).
The effects of fluoride-containing toothpaste has been more extensive. A 2017 meta-analysis of 96 randomized controlled trials, including more than 65,000 participants, found tooth brushing with a fluoridated toothpaste reduced caries in primary teeth of children and in permanent teeth of adults compared to brushing with non-fluoridated toothpaste (24). In participants overall, use of toothpastes containing 1,000 to 1,500 ppm of fluoride had a caries-preventative effect compared to use of toothpastes with lower fluoride concentrations or with non-fluoridated toothpastes (24). A systematic review of 17 clinical trials found use of fluoridated toothpaste effectively reduced dental caries in primary teeth of children younger than 6 years who were at high risk of developing dental caries (25).
The attack of dental hard tissue by acids other than those produced by the bacterial plaque may lead to the loss of tooth enamel, also known as dental erosion. Factors involved in dental erosion include acidic foods and beverages (e.g., carbonated drinks) and acid reflux (26). The protective effect of fluoridated agents against dental erosion has mainly been observed in in vitro studies (reviewed in 26). Nevertheless, a meta-analysis of four small, randomized trials examining the effect of fluoride in toothpaste, varnish, and saliva on dental erosion did not find any overall benefit compared to placebo (27). Larger clinical studies are needed to evaluate whether topical fluoride applications can prevent dental erosion and/or reduce the progression of existing erosive lesions.
Although fluoride in pharmacologic doses has been shown to be a potent therapeutic agent for increasing spinal bone mass (see Disease Treatment), there is little evidence that water fluoridation at optimum levels for the prevention of dental caries is helpful in the prevention of osteoporosis. The majority of studies conducted to date have failed to find clinically significant differences in bone mineral density (BMD) or fracture incidence when comparing residents of areas with fluoridated water supplies to residents in areas without fluoridated water supplies (28, 29). However, two studies found that drinking water fluoridation was associated with decreased incidence of hip fracture in the elderly. In addition, one study in Italy found a significantly greater risk of femoral (hip) fractures in men and women residing in an area with low water fluoridation (0.05 ppm) compared to the risk in a similar population whose water supply was naturally fluoridated (1.45 ppm) at higher than optimum levels for prevention of dental caries (30). Another study in Germany found no significant difference in BMD between residents of a community whose water supply had been optimally fluoridated for 30 years (1 ppm) compared with those who resided in a community without fluoridated water. However, this study reported that the incidence of hip fracture in men and women, aged 85 years or older, was significantly lower in the community with fluoridated water compared to the community with non-fluoridated water, despite higher calcium levels in the non-fluoridated water supply (31). Another community-based study in 1,300 women found that elevated serum fluoride concentrations were not related to BMD or to osteoporotic fracture incidence (32). Finally, a nationwide cohort study in Sweden found no association between chronic exposure to fluoridated water and incidence of hip fracture (33). A 2015 meta-analysis, which pooled results of 13 prospective cohort studies and one case-control study, found that fluoride exposure in drinking water was not associated with risk of hip fracture (34).
Moreover, because bone mineral accretion early in life affects risk for osteoporosis in later adulthood, studies have examined the association of fluoride intake during adolescence and bone outcomes. Reports from the Iowa Bone Development Study, an ongoing prospective cohort study, indicate little to no association of fluoride intake during childhood and adolescence with measures of bone microstructure throughout adolescence (35-37) and into early adulthood (38).
Osteoporosis is characterized by decreased bone mineral density (BMD) and increased bone fragility and susceptibility to fracture. In general, decreased BMD is associated with increased risk of fracture. However, the usual relationship between BMD and fracture risk does not always hold true when very high (pharmacologic) doses of fluoride are used to treat osteoporosis. Most available therapies for osteoporosis (e.g., estrogen, calcitonin, and bisphosphonates) decrease bone loss (resorption), resulting in very small increases in BMD. Pharmacologic doses of fluoride are capable of producing large increases in the BMD of the lumbar spine. Overall, therapeutic trials of fluoride in patients with osteoporosis have not consistently demonstrated significant decreases in the occurrence of vertebral fracture despite dramatic increases in lumbar spine BMD (39). A meta-analysis of 11 controlled studies, including 1,429 participants, found that fluoride treatment resulted in increased BMD at the lumbar spine but was not associated with a lower risk of vertebral fractures (40). This meta-analysis also found that higher concentrations of fluoride were associated with increased risk of non-vertebral fractures after four years of treatment. Early studies using high doses of fluoride (>20 mg/day) may have induced rapid bone mineralization in the absence of adequate calcium and vitamin D, resulting in denser bones that were not mechanically stronger (41, 42). Analysis of bone architecture has also shed some light on the inconsistent effect of fluoride therapy in reducing vertebral fractures. Research has indicated that osteoporosis may be associated with an irreversible change in the architecture of bone known as decreased trabecular connectivity. Normal bone consists of a series of plates interconnected by thick rods. Severely osteoporotic bone has fewer plates, and the rods may be fractured or disconnected (decreased trabecular connectivity) (43). Despite fluoride therapy increasing bone density, it probably cannot reduce bone resorption and restore connectivity in patients with severe bone loss. Thus, fluoride therapy may be less effective in osteoporotic individuals who have already lost substantial trabecular connectivity (39, 44).
On the other hand, randomized controlled trials using lower fluoride doses (≤20 mg/day), intermittent dosage schedules, or slow-release formulations (enteric coated sodium fluoride) have demonstrated a decreased incidence of vertebral and non-vertebral fractures along with increased bone density of the lumbar spine (45). Yet, bone biopsies from postmenopausal, osteoporotic women treated with 20 mg/day of fluoride showed evidence of abnormal bone mineralization despite calcium and vitamin D supplementation (46). Additionally, a randomized, double-blind, placebo-controlled study did not find any increase in lumbar spine BMD in 180 postmenopausal women with osteopenia (early osteoporosis) who were given daily supplements of up to 10 mg/day of fluoride for one year (47). Additional studies are required to assess whether a safe dose of fluoride can be found to maximize bone formation while preventing mineralization defects.
Serious side effects have been associated with the high doses of fluoride used to treat osteoporosis (45). They include gastrointestinal irritation, joint pain in the lower extremities, and the development of calcium deficiency and stress fractures. The reasons for the occurrence of lower extremity joint pain and stress fractures in patients taking fluoride for osteoporosis remain unclear, but they may be related to rapid increases in bone formation without sufficient calcium to support such an increase (39). Presently, enteric coated sodium fluoride or monofluorophosphate preparations offer a lower side effect profile than the high-dose sodium fluoride used in earlier trials. Additionally, sufficient calcium and vitamin D must be provided to support fluoride-induced bone formation. Although fluoride therapy may be beneficial for the treatment of osteoporosis in appropriately selected and closely monitored individuals, uncertainty about its safety and benefit in reducing fractures has kept the US Food and Drug Administration (FDA) from approving fluoride therapy for osteoporosis (48). Combinations of lower doses of fluoride with antiresorptive agents, such as estrogen or bisphosphonates, may improve therapeutic results while minimizing side effects (49, 50). Yet, randomized studies have shown that the risk of fractures remained unchanged whether treatments include fluoride, antiresorptives, or both (45, 46). Additional studies are warranted to determine whether any treatment combinations could provide substantial therapeutic benefits over monotherapy.
The major source of dietary fluoride in the US diet is drinking water. Controlled addition of fluoride to water is used by communities as a public health measure to adjust fluoride concentration in drinking water to prevent dental caries. Originally, an optimal range of 0.7 to 1.2 milligrams (mg) per liter (corresponding to 0.7-1.2 ppm) was established, which was shown to decrease the incidence of dental caries while minimizing the risk of dental fluorosis and other adverse effects. In 2015, the US Department of Health and Human Services recommended that the optimal concentration in drinking water be set at 0.7 ppm (see Safety) (51). Approximately 73% of the US population receives water with sufficient fluoride for the prevention of dental caries (52). The average fluoride intake for adults living in fluoridated communities ranges from 1.4 to 3.4 mg/day compared to 0.3 to 1 mg/day in non-fluoridated areas (6). Since well water can vary greatly in its fluoride content, people who consume water from wells should have the fluoride content of their water tested by their local water district or health department. Water fluoride testing may also be warranted in households that use home water treatment systems. While water softeners are not thought to change water fluoride levels, reverse osmosis systems, distillation units, and some water filters have been found to remove significant amounts of fluoride from water. However, Brita-type carbon-charcoal filters do not remove fluoride (6, 48).
Bottled water sales have grown exponentially in the US in the last decades, and studies have found that most bottled waters contain sub-optimal levels of fluoride, although there is considerable variation (53). For example, a study of 105 different bottled water products in the Greater Houston metropolitan area found that over 80% had fluoride concentrations of less than 0.4 ppm; only 5% of the tested products had fluoride concentrations within the recommended range (54). Several other studies have reported similar findings, with most bottled waters relatively low in fluoride, but a few in the optimal range or higher (55-57). The FDA-approved claim that "drinking fluoridated water may reduce the risk of tooth decay" is only used by bottlers when the water contains greater than 0.6 ppm of fluoride but no more than 1.0 ppm of fluoride. However, bottlers are not required to provide the fluoride concentration in bottled water unless fluoride was added (58).
While consumption of fluoride from water presents very little risk of adverse effects in adults except in extreme circumstances (see Safety), consumption of relatively large amounts of water mixed with formula concentrates appears to increase the risk for the development of dental fluorosis in infants (59-61). One study found that, on average, at least half of all fluoride ingested by infants 6 months and younger was from water mixed with formula concentrates (62). The study of 49 commercially available infant formulas in the Chicago area showed that milk-based ready-to-feed, liquid concentrate, and powdered formulas (reconstituted with deionized water) had mean fluoride concentrations of 0.15 ppm, 0.27 ppm, and 0.12 ppm, respectively (63). Fluoride content was significantly higher in soy-based compared to milk-based liquid concentrate formulas (0.50 ppm vs. 0.27 ppm). Using average body weights and total formula intakes during the first year of life, the authors estimated that the risk of exceeding the tolerable upper intake level (UL) for fluoride ingestion was minimal when liquid concentrate and powdered formulas were reconstituted with water containing less than 0.5 ppm of fluoride, but the risk was maximal with 1.0 ppm fluoridated water. Fluoride-free or low-fluoride water labeled as "deionized," "purified," "demineralized," "distilled," or "produced through reverse-osmosis" can be used in order to minimize the risk for mild fluorosis (58). However, infants between 6 and 12 months may not reach the adequate intake of fluoride if they are fed ready-to-feed formulas or formulas reconstituted with water containing less than 0.4 ppm (63).
For additional information on fluoride and infant formulas, see the CDC website.
The fluoride content of most foods is low (less than 0.05 mg/100 grams or 0.5 ppm). Rich sources of fluoride include tea, which concentrates fluoride in its leaves, and marine fish that are consumed with their bones (e.g., sardines). Foods made with mechanically separated (boned) chicken, such as canned meats, hot dogs, and infant foods, also add fluoride to the diet (64). In addition, certain fruit juices, particularly grape juices, often have relatively high fluoride concentrations (65). Foods generally contribute only 0.3-0.6 mg of the daily intake of fluoride. An adult male residing in a community with fluoridated water has an intake range from 1 mg/day-3 mg/day. Intake is less than 1 mg/day in non-fluoridated areas (2). Table 2 provides a range of fluoride content for a few fluoride-rich foods. For more information on the fluoride content of foods and beverages, search the USDA national fluoride database.
Fluoride supplements — available only by prescription in the US — are intended for infants 6 months and older and children up to 16 years of age living in areas with suboptimal water fluoridation for the purpose of bringing their intake to approximately 1 mg/day (6). The American Dental Association Council on Scientific Affairs recommends the prescription of fluoride supplements only to children at high risk of developing dental caries (66). The supplemental fluoride dosage schedule in Table 3 was recommended by the American Dental Association, the American Academy of Pediatric Dentistry, and the American Academy of Pediatrics (66, 67). It requires knowledge of the fluoride concentration of local drinking water, as well as other possible sources of fluoride intake. For more detailed information regarding fluoride and the prevention of dental caries, visit the American Dental Association website.
Fluoridated toothpastes (1,000-1,100 ppm of fluoride) are very effective in preventing dental caries but also add considerably to fluoride intake of children, especially young children who are more likely to swallow toothpaste. Researchers estimate that children under 6 years of age may ingest an average of 0.3 mg of fluoride from toothpaste with each brushing. Children under the age of 6 years who ingest more than two or three times the recommended fluoride intake are at increased risk of a white speckling or mottling of the permanent teeth, known as dental fluorosis (see Safety section below). A major source of excess fluoride intake in this age group comes from swallowing fluoride-containing toothpaste. To prevent dental fluorosis while providing optimum protection from tooth decay, it is recommended that parents supervise children under 6 years of age while brushing with fluoridated toothpaste. In addition to discouraging the swallowing of toothpaste, children should be supervised during teeth brushing, and young children should be encouraged to use very small amounts of toothpaste — a "smear amount" (a thin layer of toothpaste that covers less than half of the bristle surface of a child-size toothbrush; size equivalent to a grain of rice) for children younger than 3 years, and no more than a pea-sized application of toothpaste for children 3 to 6 years of age (25, 68-70). Interestingly, it has been suggested that the management of the fluorosis risk in young children who ingest fluoridated toothpaste could include the use of toothpaste formulation that reduces gastrointestinal absorption and bioavailability of fluoride (71).
Fluoridation of salt has been implemented in several countries worldwide as an alternative to water fluoridation to promote the ingestion of fluoride and improve oral care. Since the fluoridation of water is extensively practiced in the US, fluoride is not added to salt. Observational studies have shown that the incidence of teeth with caries dramatically decreased in the regions where salt fluoridation programs were developed (reviewed in 72). While concerns around hypertension and the monitoring of population intakes should be addressed, no adverse health effects linked to the fluoridation of salt have been reported (reviewed in 73). According to the World Health Organization (WHO), salt fluoridation and, to a lesser extent, milk fluoridation, are affordable alternatives to improve oral hygiene in areas where access to oral health services is limited and fluoridation of public water is not feasible (74).
Mouth rinses that contain fluoride are available over-the-counter in the US. Such products often contain 0.05% sodium fluoride, which translates to about 1 mg of fluoride per 5 mL (one teaspoon) (70). Due to the risk of accidental ingestion, fluoride-containing mouth rinses are not recommended for young children (70).
Professionally applied fluoride products, including fluoride foams, gels, varnish, and silver diamine fluoride, are highly concentrated (9,000 to 44,800 ppm of fluoride) and applied topically to the teeth by dentists, dental hygienists, or other healthcare professionals (75). Because of their high concentrations, they are potential sources of fluoride; however, due to their infrequent use (every 3-6 months) and small amounts used per application, professionally applied fluoride products are not significant sources of fluoride when used as directed (75).
Fluoridation of public drinking water in the US was initiated more than 70 years ago. Since then, a number of adverse effects have been attributed to water fluoridation. However, extensive scientific research has uncovered no evidence of increased risks of cancer, heart disease, kidney disease, liver disease, thyroid disease, Alzheimer's disease, birth defects, or Down's syndrome (51, 76, 77).
A number of observational studies, mostly published in Chinese journals, have investigated the association between fluoride content in drinking water and children’s neurodevelopment. Two meta-analyses of observational studies, mainly conducted in China, found lower intelligence quotients (IQs) in children exposed to higher fluoride concentrations in drinking water (78, 79). Serious limitations, including substantial heterogeneity among studies and co-occurrence of neurotoxicants in drinking water, hinder the strength of these findings and their application to US settings. The Academy of Nutrition and Dietetics has estimated that only limited evidence supports an association between fluoride content in water and the IQs of children (58). A prospective study in a New Zealand population-based cohort followed for nearly four decades found no association between fluoride exposure in the context of community water fluoridation programs and IQs measured during childhood and at age 38 years (80). A series of recent studies by a research group in Canada have raised concern over a possible link between higher maternal fluoride exposures during pregnancy and lower IQ (81-83), cognitive delay (84), and attention-deficit/hyperactivity disorder (85) in offspring. However, these studies have been widely criticized for shortcomings in measuring fluoride intake, only reporting significant relationships among subgroups, and being observational and subject to residual confounding. Thus, high-quality prospective studies with more definitive fluoride intake measures and better control of confounders are needed to determine whether fluoride might have neurotoxic effects at usual intake levels.
Fluoride is toxic when consumed in excessive amounts, so concentrated fluoride products should be used and stored with caution to prevent the possibility of acute fluoride poisoning, especially in children and other vulnerable individuals. The lowest dose that could trigger adverse symptoms is considered to be 5 mg/kg of body weight, with the lowest potentially fatal dose considered 15 mg/kg of body weight. Nausea, abdominal pain, and vomiting almost always accompany acute fluoride toxicity. Other symptoms like diarrhea, excessive salivation and tearing, sweating, and generalized weakness may also occur (77). In order to prevent acute fluoride poisoning, the American Dental Association has recommended that no more than 120 mg of fluoride (224 mg of sodium fluoride) be dispensed at one time (48). The use of high doses of fluoride to treat osteoporosis has been associated with some adverse effects, which are discussed in the Disease Treatment section above.
Dental fluorosis, also called enamel fluorosis, is a result of excess fluoride intake during the period of tooth formation, with the critical window of susceptibility being the first eight years of life, as this corresponds to the eruption of the permanent teeth (86). Once the tooth enamel has formed, dental fluorosis cannot develop (87). The mildest form of dental fluorosis is detectable only to the trained observer and is characterized by small opaque white flecks or spots on the enamel of the teeth. Moderate dental fluorosis is characterized by mottling and mild staining of the teeth, and severe dental fluorosis results in marked staining and pitting of the teeth. In its moderate to severe forms, dental fluorosis becomes a cosmetic concern when it affects the incisors and canines (front teeth). Dental fluorosis is a dose-dependent condition, with higher fluoride intakes being associated with more pronounced effects on the teeth.
The incidence of mild and moderate dental fluorosis has increased over the past decades, mainly due to increasing fluoride intake from reconstituted infant formula and toothpaste, although inappropriate use of fluoride supplements may also contribute (61). According to a US national survey, the National Health and Nutrition Examination Survey (NHANES) 1999-2004, 23% of people aged 6 to 49 years (n=16,051) had some degree of dental fluorosis (88). National data from NHANES 2011-2012 found that the prevalence of fluorosis among children and adolescents (n=2,283), ages 6 to 19 years, was much higher at 57% (89); however, a quality assessment of these data raised concerns about their validity and suggested such results were not biologically plausible (90). In 1997, the US Food and Nutrition Board (FNB) of the Institute of Medicine set the tolerable upper intake level (UL) for fluoride based on the prevention of moderate enamel fluorosis (Table 4) (6).
The current US EPA maximum allowable level of fluoride in drinking water is 4 mg/L; the EPA also has a non-enforceable standard fluoride level of 2 mg/L to prevent moderate dental fluorosis (91). The EPA recently conducted a six-year review of drinking water standards and concluded that the limit of fluoride in drinking water is not a candidate for regulatory revision at this time (92).
Intake of fluoride at excessive levels for long periods of time may lead to changes in bone structure known as skeletal fluorosis. The early stages of skeletal fluorosis are characterized by increased bone mass, detectable by x-ray. If very high fluoride intake persists over many years, joint pain and stiffness may result from the skeletal changes. The most severe form of skeletal fluorosis is known as "crippling skeletal fluorosis," which may result in calcification of ligaments, immobility, muscle wasting, and neurological problems related to spinal cord compression. While skeletal fluorosis is endemic in many world regions with naturally high fluoride concentrations in drinking water, crippling skeletal fluorosis may occur only when fluoride intake exceeds 10 mg/day for at least 10 years (6, 93). Rare cases of skeletal fluorosis in the US have been observed in consumers of large volumes of tea (94-97). Because of the potential risk for skeletal fluorosis, as well as the risks for pitting of tooth enamel and bone fracture, the US EPA set the maximum level of fluoride allowed in drinking water at 4 mg/L (98). The agency also recommended limiting fluoride in drinking water at 2 mg/L to prevent dental fluorosis in children; however, this is only a guideline and not enforceable by law (see the US EPA website).
Calcium supplements, as well as calcium and aluminum-containing antacids, can decrease the absorption of fluoride. It is best to take these products two hours before or after fluoride supplements (99).
The safety and public health benefits of optimally fluoridated water for prevention of tooth decay in people of all ages have been well established. The Linus Pauling Institute supports the recommendations of the American Dental Association and the Centers for Disease Control and Prevention, which include optimally fluoridated water and the use of fluoride toothpaste, fluoride mouth rinse, fluoride varnish, and when necessary, fluoride supplementation. Due to the risk of fluorosis, any fluoride supplementation should be prescribed and closely monitored by a dentist or physician.
Originally written in 2001 by:
Jane Higdon, Ph.D.
Linus Pauling Institute
Oregon State University
Updated in April 2003 by:
Jane Higdon, Ph.D.
Linus Pauling Institute
Oregon State University
Updated in September 2007 by:
Victoria J. Drake, Ph.D.
Linus Pauling Institute
Oregon State University
Updated in November 2013 by:
Barbara Delage, Ph.D.
Linus Pauling Institute
Oregon State University
Updated in November 2021 by:
Victoria J. Drake, Ph.D.
Linus Pauling Institute
Oregon State University
Reviewed in December 2021 by:
John J. Warren, D.D.S., M.S.
Professor
Preventive & Community Dentistry
College of Dentistry
The University of Iowa
Copyright 2001-2024 Linus Pauling Institute
1. Cerklewski FL. Fluoride bioavailability — nutritional and clinical aspects. Nutr Res. 1997;17:907-929.
2. Nielsen FH. Ultratrace minerals. In: Shils M, Olson JA, Shike M, Ross AC, eds. Modern Nutrition in Health and Disease. 9th ed. Baltimore: Williams & Wilkins; 1999:283-303.
3. Cerklewski FL. Fluoride — essential or just beneficial. Nutrition. 1998;14(5):475-476. (PubMed)
4. Cerklewski FL. Fluorine. In: O'Dell BL, Sunde RA, eds. Handbook of Nutritionally Essential Minerals. New York: Marcel Dekker, Inc.; 1997:583-602.
5. US Department of Health Human Services Federal Panel on Community Water Fluoridation. US Public Health Service Recommendation for Fluoride Concentration in Drinking Water for the Prevention of Dental Caries. Public Health Rep. 2015;130(4):318-331. (PubMed)
6. Food and Nutrition Board, Institute of Medicine. Fluoride. Dietary Reference Intakes: Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington D.C.: National Academy Press; 1997:288-313. (National Academy Press)
7. US Centers for Disease Control and Prevention. Achievements in public health, 1900-1999: fluoridation of drinking water to prevent dental caries. MMWR. 1999;48:933-940.
8. Demmer RT, Squillaro A, Papapanou PN, et al. Periodontal infection, systemic inflammation, and insulin resistance: results from the continuous National Health and Nutrition Examination Survey (NHANES) 1999-2004. Diabetes Care. 2012;35(11):2235-2242. (PubMed)
9. Demmer RT, Jacobs DR, Jr., Desvarieux M. Periodontal disease and incident type 2 diabetes: results from the First National Health and Nutrition Examination Survey and its epidemiologic follow-up study. Diabetes Care. 2008;31(7):1373-1379. (PubMed)
10. Desvarieux M, Demmer RT, Jacobs DR, Jr., et al. Periodontal bacteria and hypertension: the oral infections and vascular disease epidemiology study (INVEST). J Hypertens. 2010;28(7):1413-1421. (PubMed)
11. Bahekar AA, Singh S, Saha S, Molnar J, Arora R. The prevalence and incidence of coronary heart disease is significantly increased in periodontitis: a meta-analysis. Am Heart J. 2007;154(5):830-837. (PubMed)
12. Kriauciunas A, Gleiznys A, Gleiznys D, Januzis G. The influence of Porphyromonas gingivalis bacterium causing periodontal disease on the pathogenesis of rheumatoid arthritis: systematic review of literature. Cureus. 2019;11(5):e4775. (PubMed)
13. Perricone C, Ceccarelli F, Saccucci M, et al. Porphyromonas gingivalis and rheumatoid arthritis. Curr Opin Rheumatol. 2019;31(5):517-524. (PubMed)
14. Batty GD, Jung KJ, Mok Y, et al. Oral health and later coronary heart disease: Cohort study of one million people. Eur J Prev Cardiol. 2018;25(6):598-605. (PubMed)
15. Demmer RT, Desvarieux M. Periodontal infections and cardiovascular disease: the heart of the matter. J Am Dent Assoc. 2006;137 Suppl:14S-20S; quiz 38S. (PubMed)
16. Zoellner H. Dental infection and vascular disease. Semin Thromb Hemost. 2011;37(3):181-192. (PubMed)
17. DePaola DP, Faine MP, Palmer CA. Nutrition in relation to dental medicine. In: Shils M, Olson JA, Shike M, Ross AC, eds. Modern Nutrition in Health and Disease. 9th ed. Baltimore: Williams & Wilkins; 1999:1099-1124.
18. Whelton HP, Spencer AJ, Do LG, Rugg-Gunn AJ. Fluoride revolution and dental caries: evolution of policies for global use. J Dent Res. 2019;98(8):837-846. (PubMed)
19. Newbrun E. Effectiveness of water fluoridation. J Public Health Dent. 1989;49(5 Spec No):279-289. (PubMed)
20. Iheozor-Ejiofor Z, Worthington HV, Walsh T, et al. Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev. 2015(6):CD010856. (PubMed)
21. Dye BA, Tan S, Smith V, Lewis BG, Barker LK, Thornton-Evans G. Trends in oral health status: United States, 1988-1994 and 1999-2004. National Center for Health Statistics. Vital Health Stat 11(248); 2007.
22. Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013;7:CD002279. (PubMed)
23. Chou R, Pappas M, Dana T, et al. Screening and interventions to prevent dental caries in children younger than 5 years: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;326(21):2179-2192. (PubMed)
24. Walsh T, Worthington HV, Glenny AM, Marinho VC, Jeroncic A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev. 2019;3:CD007868. (PubMed)
25. Wright JT, Hanson N, Ristic H, Whall CW, Estrich CG, Zentz RR. Fluoride toothpaste efficacy and safety in children younger than 6 years: a systematic review. J Am Dent Assoc. 2014;145(2):182-189. (PubMed)
26. Magalhaes AC, Wiegand A, Rios D, Honorio HM, Buzalaf MA. Insights into preventive measures for dental erosion. J Appl Oral Sci. 2009;17(2):75-86. (PubMed)
27. Zini A, Krivoroutski Y, Vered Y. Primary prevention of dental erosion by calcium and fluoride: a systematic review. Int J Dent Hyg. 2014;12(1):17-24. (PubMed)
28. Krall EA, Dawson-Hughes B. Osteoporosis. In: Shils M, Olson JA, Shike M, Ross AC, eds. Modern Nutrition in Health and Disease. 9th ed. Baltimore: Williams & Wilkins; 1999:1353-1364.
29. Lee N, Kang S, Lee W, Hwang SS. The association between community water fluoridation and bone diseases: a natural experiment in Cheongju, Korea. Int J Environ Res Public Health. 2020;17(24):9170. (PubMed)
30. Fabiani L, Leoni V, Vitali M. Bone-fracture incidence rate in two Italian regions with different fluoride concentration levels in drinking water. J Trace Elem Med Biol. 1999;13(4):232-237. (PubMed)
31. Lehmann R, Wapniarz M, Hofmann B, Pieper B, Haubitz I, Allolio B. Drinking water fluoridation: bone mineral density and hip fracture incidence. Bone. 1998;22(3):273-278. (PubMed)
32. Sowers M, Whitford GM, Clark MK, Jannausch ML. Elevated serum fluoride concentrations in women are not related to fractures and bone mineral density. J Nutr. 2005;135(9):2247-2252. (PubMed)
33. Nasman P, Ekstrand J, Granath F, Ekbom A, Fored CM. Estimated drinking water fluoride exposure and risk of hip fracture: a cohort study. J Dent Res. 2013;92(11):1029-1034. (PubMed)
34. Yin XH, Huang GL, Lin DR, et al. Exposure to fluoride in drinking water and hip fracture risk: a meta-analysis of observational studies. PLoS One. 2015;10(5):e0126488. (PubMed)
35. Levy SM, Eichenberger-Gilmore J, Warren JJ, et al. Associations of fluoride intake with children's bone measures at age 11. Community Dent Oral Epidemiol. 2009;37(5):416-426. (PubMed)
36. Levy SM, Warren JJ, Phipps K, et al. Effects of life-long fluoride intake on bone measures of adolescents: a prospective cohort study. J Dent Res. 2014;93(4):353-359. (PubMed)
37. Oweis RR, Levy SM, Eichenberger-Gilmore JM, et al. Fluoride intake and cortical and trabecular bone characteristics in adolescents at age 17: A prospective cohort study. Community Dent Oral Epidemiol. 2018;46(6):527-534. (PubMed)
38. Saha PK, Oweis RR, Zhang X, et al. Effects of fluoride intake on cortical and trabecular bone microstructure at early adulthood using multi-row detector computed tomography (MDCT). Bone. 2021;146:115882. (PubMed)
39. Cesar Libanati K-H. Fluoride therapy for osteoporosis. In: Marcus R, ed. Osteoporosis. San Diego: Academic Press; 1996:1259-1277.
40. Haguenauer D, Welch V, Shea B, Tugwell P, Adachi JD, Wells G. Fluoride for the treatment of postmenopausal osteoporotic fractures: a meta-analysis. Osteoporos Int. 2000;11(9):727-738. (PubMed)
41. Riggs BL, Hodgson SF, O'Fallon WM, et al. Effect of fluoride treatment on the fracture rate in postmenopausal women with osteoporosis. N Engl J Med. 1990;322(12):802-809. (PubMed)
42. Lundy MW, Stauffer M, Wergedal JE, et al. Histomorphometric analysis of iliac crest bone biopsies in placebo-treated versus fluoride-treated subjects. Osteoporos Int. 1995;5(2):115-129. (PubMed)
43. Fields AJ, Keaveny TM. Trabecular architecture and vertebral fragility in osteoporosis. Curr Osteoporos Rep. 2012;10(2):132-140. (PubMed)
44. Balena R, Kleerekoper M, Foldes JA, et al. Effects of different regimens of sodium fluoride treatment for osteoporosis on the structure, remodeling and mineralization of bone. Osteoporos Int. 1998;8(5):428-435. (PubMed)
45. Vestergaard P, Jorgensen NR, Schwarz P, Mosekilde L. Effects of treatment with fluoride on bone mineral density and fracture risk — a meta-analysis. Osteoporos Int. 2008;19(3):257-268. (PubMed)
46. Reid IR, Cundy T, Grey AB, et al. Addition of monofluorophosphate to estrogen therapy in postmenopausal osteoporosis: a randomized controlled trial. J Clin Endocrinol Metab. 2007;92(7):2446-2452. (PubMed)
47. Grey A, Garg S, Dray M, et al. Low-dose fluoride in postmenopausal women: a randomized controlled trial. J Clin Endocrinol Metab. 2013;98(6):2301-2307. (PubMed)
48. American Dietetic Association. Position of the American Dietetic Association: the impact of fluoride on health. J Am Diet Assoc. 2001;101(1):126-132. (PubMed)
49. Murray TM, Ste-Marie LG. Prevention and management of osteoporosis: consensus statements from the Scientific Advisory Board of the Osteoporosis Society of Canada. 7. Fluoride therapy for osteoporosis. CMAJ. 1996;155(7):949-954. (PubMed)
50. Alexandersen P, Riis BJ, Christiansen C. Monofluorophosphate combined with hormone replacement therapy induces a synergistic effect on bone mass by dissociating bone formation and resorption in postmenopausal women: a randomized study. J Clin Endocrinol Metab. 1999;84(9):3013-3020. (PubMed)
51. US Department of Health and Human Services Federal Panel on Community Water Fluoridation. US Public health service recommendation for fluoride concentration in drinking water for the prevention of dental caries. Public Health Rep. 2015;130(4):318-31. (PubMed)
52. US Centers for Disease Control and Prevention. Community Water Fluoridation. Water Floridation Basics. Available at: https://www.cdc.gov/fluoridation/basics/index.htm. Accessed 11/19/21.
53. Cutrufelli R, Pehrsson P, Haytowitz D, Patterson K, Holden J. USDA National Fluoride Database of Selected Beverages and Foods, Release 2. Nutrient Data Laboratory, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S. Department of Agriculture; 2005.
54. Quock RL, Chan JT. Fluoride content of bottled water and its implications for the general dentist. Gen Dent. 2009;57(1):29-33. (PubMed)
55. Van Winkle S, Levy SM, Kiritsy MC, Heilman JR, Wefel JS, Marshall T. Water and formula fluoride concentrations: significance for infants fed formula. Pediatr Dent. 1995;17(4):305-310. (PubMed)
56. Tate WH, Chan JT. Fluoride concentrations in bottled and filtered waters. Gen Dent. 1994;42(4):362-366. (PubMed)
57. McGuire S. Fluoride content of bottled water. N Engl J Med. 1989;321(12):836-837. (PubMed)
58. Palmer CA, Gilbert JA, Academy of N, Dietetics. Position of the Academy of Nutrition and Dietetics: the impact of fluoride on health. J Acad Nutr Diet. 2012;112(9):1443-1453. (PubMed)
59. Marshall TA, Levy SM, Warren JJ, Broffitt B, Eichenberger-Gilmore JM, Stumbo PJ. Associations between Intakes of fluoride from beverages during infancy and dental fluorosis of primary teeth. J Am Coll Nutr. 2004;23(2):108-116. (PubMed)
60. Pendrys DG. Risk of enamel fluorosis in nonfluoridated and optimally fluoridated populations: considerations for the dental professional. J Am Dent Assoc. 2000;131(6):746-755. (PubMed)
61. Levy SM, Broffitt B, Marshall TA, Eichenberger-Gilmore JM, Warren JJ. Associations between fluorosis of permanent incisors and fluoride intake from infant formula, other dietary sources and dentifrice during early childhood. J Am Dent Assoc. 2010;141(10):1190-1201. (PubMed)
62. Levy SM, Kohout FJ, Guha-Chowdhury N, Kiritsy MC, Heilman JR, Wefel JS. Infants' fluoride intake from drinking water alone, and from water added to formula, beverages, and food. J Dent Res. 1995;74(7):1399-1407. (PubMed)
63. Siew C, Strock S, Ristic H, et al. Assessing a potential risk factor for enamel fluorosis: a preliminary evaluation of fluoride content in infant formulas. J Am Dent Assoc. 2009;140(10):1228-1236. (PubMed)
64. Fein NJ, Cerklewski FL. Fluoride content of foods made with mechanically separated chicken. J Agric Food Chem. 2001;49(9):4284-4286. (PubMed)
65. Kiritsy MC, Levy SM, Warren JJ, Guha-Chowdhury N, Heilman JR, Marshall T. Assessing fluoride concentrations of juices and juice-flavored drinks. J Am Dent Assoc. 1996;127(7):895-902. (PubMed)
66. Rozier RG, Adair S, Graham F, et al. Evidence-based clinical recommendations on the prescription of dietary fluoride supplements for caries prevention: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2010;141(12):1480-1489. (PubMed)
67. US Centers for Disease Control and Prevention. Recommendations for using fluoride to prevent and control dental caries in the United States. MMWR Recomm Rep. 2001;50(RR-14):1-42.
68. Section on Pediatric Dentistry and Oral Health. Preventive oral health intervention for pediatricians. Pediatrics. 2008;122(6):1387-1394. (PubMed)
69. American Dental Association Council on Scientific Affairs. Fluoride toothpaste use for young children. J Am Dent Assoc. 2014;145(2):190-191. (PubMed)
70. Clark MB, Keels MA, Slayton RL, Section On Oral Health. Fluoride use in caries prevention in the primary care setting. Pediatrics. 2020;146(6): e2020034637. (PubMed)
71. Falcao A, Tenuta LM, Cury JA. Fluoride gastrointestinal absorption from Na2FPO3/CaCO3- and NaF/SiO2-based toothpastes. Caries Res. 2013;47(3):226-233. (PubMed)
72. O'Mullane DM, Baez RJ, Jones S, et al. Fluoride and oral health. Community Dent Health. 2016;33(2):69-99. (PubMed)
73. Pollick HF. Salt fluoridation: a review. J Calif Dent Assoc. 2013;41(6):395-397, 400-394. (PubMed)
74. Marthaler TM, Petersen PE. Salt fluoridation — an alternative in automatic prevention of dental caries. Int Dent J. 2005;55(6):351-358. (PubMed)
75. Moss ME, Zero DT. Fluoride and Caries Prevention. In: Mascarenhas AK, Okunseri C, Dye BA, eds. Burt and Eklund’s Dentistry, Dental Practice and the Community. 7th ed. St. Louis: Elsevier; 2021:277-295.
76. Committee on Fluoride in Drinking Water National Research Council. Fluoride in drinking water: a scientific review of EPA’s Standards. Washington D.C.: National Academies Press; 2006. (The National Academies Press)
77. Whitford GM. Acute toxicity of ingested fluoride. Monogr Oral Sci. 2011;22:66-80. (PubMed)
78. Choi AL, Sun G, Zhang Y, Grandjean P. Developmental fluoride neurotoxicity: a systematic review and meta-analysis. Environ Health Perspect. 2012;120(10):1362-1368. (PubMed)
79. Duan Q, Jiao J, Chen X, Wang X. Association between water fluoride and the level of children's intelligence: a dose-response meta-analysis. Public Health. 2018;154:87-97. (PubMed)
80. Broadbent JM, Thomson WM, Ramrakha S, et al. Community Water Fluoridation and Intelligence: Prospective Study in New Zealand. Am J Public Health. 2015;105(1):72-76. (PubMed)
81. Bashash M, Thomas D, Hu H, et al. Prenatal fluoride exposure and cognitive outcomes in children at 4 and 6-12 years of age in Mexico. Environ Health Perspect. 2017;125(9):097017. (PubMed)
82. Green R, Lanphear B, Hornung R, et al. Association between maternal fluoride exposure during pregnancy and IQ scores in offspring in Canada. JAMA Pediatr. 2019;173(10):940-948. (PubMed)
83. Xu K, An N, Huang H, et al. Fluoride exposure and intelligence in school-age children: evidence from different windows of exposure susceptibility. BMC Public Health. 2020;20(1):1657. (PubMed)
84. Valdez Jimenez L, Lopez Guzman OD, Cervantes Flores M, et al. In utero exposure to fluoride and cognitive development delay in infants. Neurotoxicology. 2017;59:65-70. (PubMed)
85. Bashash M, Marchand M, Hu H, et al. Prenatal fluoride exposure and attention deficit hyperactivity disorder (ADHD) symptoms in children at 6-12 years of age in Mexico City. Environ Int. 2018;121(Pt 1):658-666. (PubMed)
86. Buzalaf MAR. Review of fluoride intake and appropriateness of current guidelines. Adv Dent Res. 2018;29(2):157-166. (PubMed)
87. Pollick H. The role of fluoride in the prevention of tooth decay. Pediatr Clin North Am. 2018;65(5):923-940. (PubMed)
88. Beltrán-Aguilar ED, Barker L, Dye BA. Prevalence and severity of dental fluorosis in the United States, 1999-2004. NCHS data brief, no 53. Hyattsville, MD: National Center for Health Statistics; 2010.
89. Neurath C, Limeback H, Osmunson B, Connett M, Kanter V, Wells CR. Dental fluorosis trends in US oral health surveys: 1986 to 2012. JDR Clin Trans Res. 2019;4(4):298-308. (PubMed)
90. National Center for Health Statistics, National Center for Chronic Disease Prevention and Health Promotion. Data quality evaluation of the dental fluorosis clinical assessment data from the National Health and Nutrition Examination Survey, 1999–2004 and 2011–2016. National Center for Health Statistics. Vital Health Stat 2(183); 2019.
91. US Environmental Protection Agency. New fluoride risk assessment and relative source contribution documents; 2011.
92. US Environmental Protection Agency. Six-year review 3 of drinking water standards. Available at: https://www.epa.gov/dwsixyearreview/six-year-review-3-drinking-water-standards. Accessed 11/22/21.
93. Whitford GM. The Metabolism and Toxicity of Fluoride. Basel: S. Karger AG; 1996.
94. Hallanger Johnson JE, Kearns AE, Doran PM, Khoo TK, Wermers RA. Fluoride-related bone disease associated with habitual tea consumption. Mayo Clin Proc. 2007;82(6):719-724. (PubMed)
95. Whyte MP, Totty WG, Lim VT, Whitford GM. Skeletal fluorosis from instant tea. J Bone Miner Res. 2008;23(5):759-769. (PubMed)
96. Izuora K, Twombly JG, Whitford GM, Demertzis J, Pacifici R, Whyte MP. Skeletal fluorosis from brewed tea. J Clin Endocrinol Metab. 2011;96(8):2318-2324. (PubMed)
97. Kakumanu N, Rao SD. Images in clinical medicine. Skeletal fluorosis due to excessive tea drinking. N Engl J Med. 2013;368(12):1140. (PubMed)
98. US Environmental Protection Agency. Fact sheet: Questions and answers on fluoride. January 2011. Available at: https://www.epa.gov/sites/default/files/2015-10/documents/2011_fluoride_questionsanswers.pdf. Accessed 11/22/21.
99. Minerals. Drug Facts and Comparisons. St. Louis: Facts and Comparisons; 2000:27-51.
If you appreciate this website, please help us maintain and update the Micronutrient Information Center. Make a gift during Oregon State University's annual giving drive.