Summary
Nutrient needs during pregnancy are increased in order to support the growth and development of the fetus while maintaining the mother’s health. This increased need is optimally met by a combination of physiological adaptations by the mother’s body and increased nutrient intake from food and dietary supplements.
For some micronutrients, such as folate, iron, iodine, and zinc, the requirement during pregnancy is substantially increased. For other micronutrients, the requirement is slightly increased (magnesium, vitamin C) or unchanged (calcium, vitamin D, vitamin E), yet it remains important to meet the recommended levels of intake for a healthy pregnancy. In the United States, several of these micronutrients are considered shortfall nutrients, meaning that insufficient amounts of these nutrients are consumed when following a stereotypical Western diet. In low-resource nations, iron, folate, vitamin A, and iodine are in scant supply and their deficiency during pregnancy can contribute to multiple adverse outcomes in the mother and newborn. Routine supplementation with folic acid (the synthetic form of folate) is universally recommended. Routine supplementation with iron is recommended in areas of the world with high rates of malnutrition and anemia; in the US and other high-resource nations, the need for iron supplementation is generally evaluated by a healthcare professional on an individual basis.
Condition Overview
Nutrient needs during pregnancy are increased. This is because the mother requires extra energy, building blocks, and cellular assistants to support the development and growth of the fetus. Increased nutrient needs during pregnancy are met by a combination of physiological adaptations and increased dietary intake by the mother.
Physiological adaptations
- Hormonal changes - hormonal changes during pregnancy help to direct nutrients to the developing fetus. Hormones like human chorionic gonadotropin (hCG), human placental lactogen (hPL), and estrogen stimulate maternal fat breakdown, increase bone turnover, and oppose the action of insulin. Overall, these changes allow glucose, amino acids, fatty acids, and micronutrients to flow to the developing fetus rather than being stored in maternal tissues.
- Increased absorption and reduced excretion - alterations in nutrient absorption and excretion also help the mother meet the increased nutrient demands of pregnancy. For example, gastrointestinal absorption of calcium, iron, zinc, and vitamin B12 are increased compared to that of nonpregnant individuals. Selenium excretion is reduced during pregnancy.
- Mobilization of mineral stores - the mother can access stores of calcium (from the skeleton) and iron (from a storage protein called ferritin) to meet the demands of the developing fetus. Maternal stores of calcium and iron can be replenished by ingesting these micronutrients at the recommended levels of intake (see the table below).
Dietary intake

- Energy (calories) - energy requirements increase by an estimated 300 kcal/day during the second and third trimesters of pregnancy, when the fetus is rapidly increasing in size. Because the requirement for most micronutrients increases more than the requirement for energy, women are advised to improve diet quality and get sufficient exercise during pregnancy in order to meet micronutrient requirements while maintaining a healthy weight. Appropriate weight gain during pregnancy (neither too little nor too much) helps to improve maternal and child health outcomes (Table 1).
- Water - The fluid found inside and around our cells, tissues, and organs is critical for our body’s ability to function — body water maintains our blood volume, helps transport nutrients and remove waste products, regulates body temperature, and is a critical component of every cell in our body. During pregnancy, extra fluid is needed to maintain the amniotic fluid that surrounds, cushions, and protects the developing fetus and to support an increase in maternal blood volume. Adequate fluid intake also helps combat fluid retention, constipation, and dehydration. The recommended intake for total water is 3 liters (12.7 cups)/day from drinking water, beverages, and food; of this amount, about 10 cups/day should come from water and other beverages.
- Macronutrients (protein, carbohydrate, fat)
- Protein - Protein needs increase by approximately 25 additional grams/day; many individuals already consume this amount of protein. Good protein sources include low-fat dairy products, lean meat and poultry, fish, eggs, legumes, nuts, and seeds.
- Carbohydrate - Carbohydrate intake should be at least 175 grams/day. The majority of carbohydrate intake should come from whole-grain breads and cereals, fruit, vegetables, and legumes.
- Fat - Consumption of the right kind of fat is important. Pregnant and nonpregnant individuals alike should replace saturated and trans fat with mono- and polyunsaturated fat from vegetable oils, nuts, and oily fish. By consuming the recommended amounts of the essential fatty acids, linoleic acid (omega-6 PUFA) and α-linolenic acid (omega-3 PUFA) (Table 2), pregnant individuals will meet their needs for other fatty acids, such as arachidonic acid, eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA).
- Micronutrients (vitamins, nutritionally essential minerals, and choline) - For several micronutrients, the recommended levels of intake are increased compared to nonpregnant individuals of the same age (Table 2). Considering that many individuals do not meet the recommended levels of intake for many micronutrients to begin with, special effort should be made to meet the higher nutrient needs of pregnancy. This includes making healthful dietary choices and possibly taking a dietary supplement under the supervision of a qualified healthcare provider.
| Weight Status | Prepregnancy BMI (kg/m2) | Estimated Weight Gain |
|---|---|---|
| Underweight | less than 18.5 | 28-40 lb (12.7-18.1 kg) |
| Normal weight | 18.5-24.9 | 25-35 lb (11.3-15.9 kg) |
| Overweight | 25-29.9 | 15-25 lb (6.8-11.3 kg) |
| Obese | 30 and greater | 11-20 lb (5.0-9.1 kg) |
| SOURCE: Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines; Rasmussen KM, Yaktine AL, editors. Weight Gain During Pregnancy: Reexamining the Guidelines. Washington (DC): National Academies Press (US); 2009. Summary. | ||
Table 2 also includes the tolerable upper intake level (UL) for pregnant adult women. The UL is the highest level of daily intake that is likely to pose no risk of adverse health effects in almost all individuals of a specified life stage. While intakes above the UL are not advised for any micronutrient, vitamin A excess during pregnancy can be particularly detrimental, causing heart defects and facial malformations in the newborn.
| Nutrient (units) | RDA or AI* Nonpregnant Adult (19-50y) | RDA or AI* Pregnant Adult | UL Pregnant Adult |
|---|---|---|---|
| Vitamins | |||
| Biotin (µg/d) | 30 | 30 | |
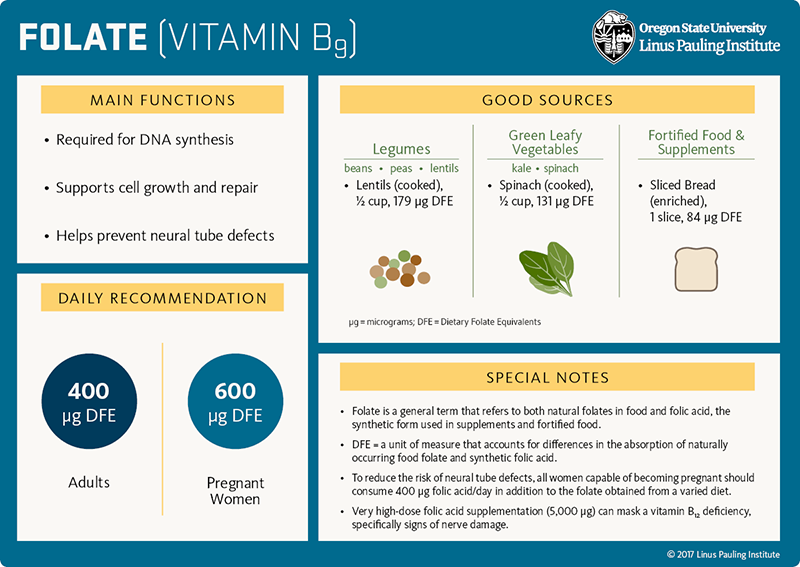
| Folate (µg/d) | 400 | 600 | 1,000 folic acid |
| Niacin (mg/d) | 14 | 18 | 35 |
| Pantothenic acid (mg/d) | 5* | 6* | |
| Riboflavin (mg/d) | 1.1 | 1.4 | |
| Thiamin (mg/d) | 1.1 | 1.4 | |
| Vitamin A (µg/day) | 700 | 770 | 3,000 |
| Vitamin B6 (mg/d) | 1.3 | 1.9 | 100 |
| Vitamin B12 (µg/d) | 2.4 | 2.6 | |
| Vitamin C (mg/d) | 75 | 85 | 2,000 |
| Vitamin D (µg/d) | 15 (600 IU) | 15 (600 IU) | 100 (4,000 IU) |
| Vitamin E (mg/d) | 15 | 15 | 1,000 |
| Vitamin K (µg/d) | 90* | 90* | |
| Minerals | |||
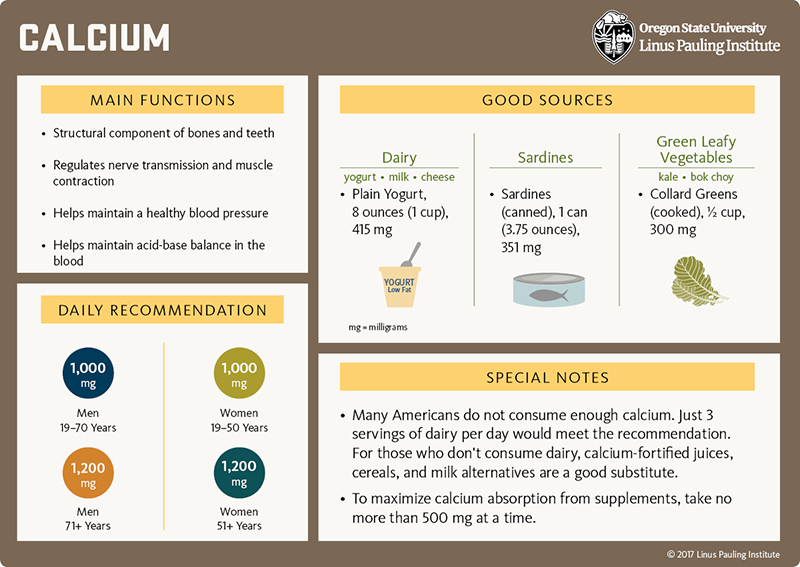
| Calcium (mg/d) | 1,000 | 1,000 | 2,500 |
| Chloride (g/d) | 2.3* | 2.3* | 3.6 |
| Chromium (µg/d) | 25* | 30* | |
| Copper (µg/d) | 900 | 1,000 | 10,000 |
| Fluoride (mg/d) | 3* | 3* | 10 |
| Iodine (µg/d) | 150 | 220 | 1,100 |
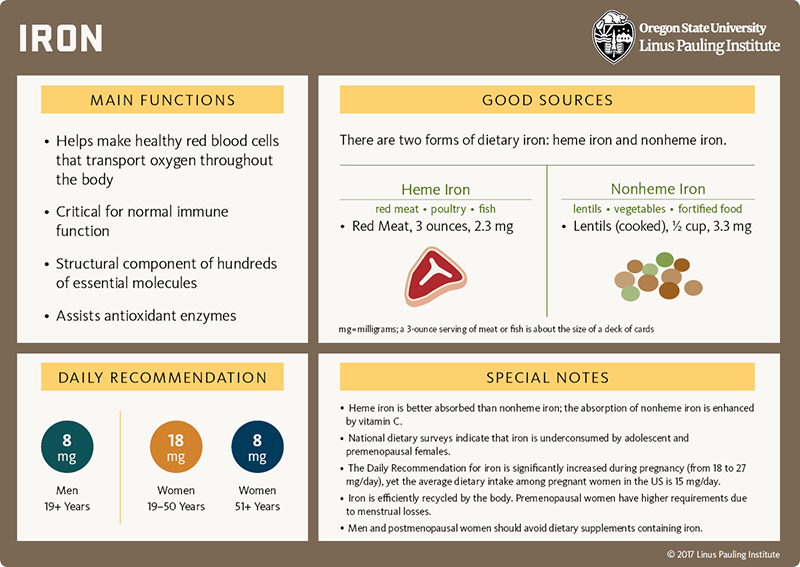
| Iron (mg/d) | 18 | 27 | 45 |
| Magnesium (mg/d) | 310 (19-30y); 320 (31-50y) | 350 | 350 supplemental magnesium |
| Manganese (mg/d) | 1.8* | 2* | 11 |
| Molybdenum (µg/d) | 45 | 50 | 2,000 |
| Phosphorus (mg/d) | 700 | 700 | 3,500 |
| Potassium (g/d) | 2.6* | 2.9* | |
| Selenium (µg/d) | 55 | 60 | 400 |
| Sodium (g/d) | 1.5* | 1.5* | |
| Zinc (mg/d) | 8 | 11 | 40 |
| Other | |||
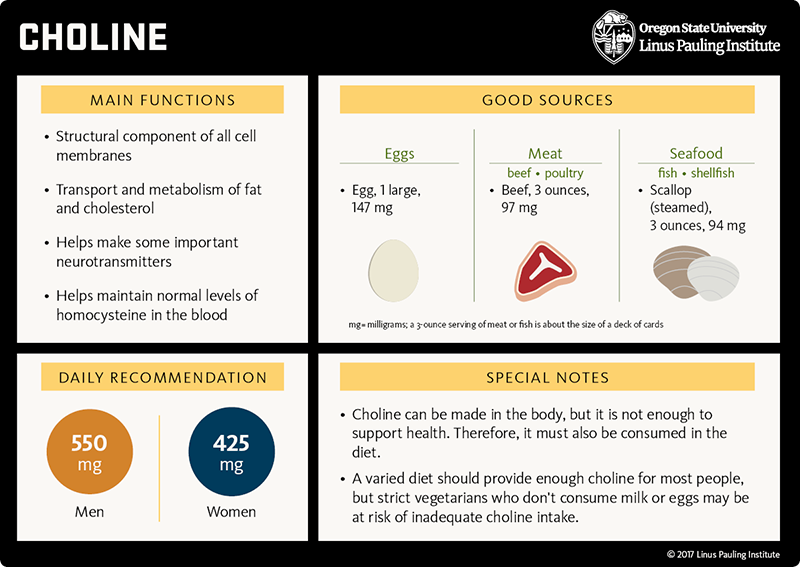
| Choline (mg/d) | 425* | 450* | 3,500 |
| n-6 PUFA, linoleic acid (g/d) | 12* | 13* | |
| n-3 PUFA, α-linolenic acid (g/d) | 1.1* | 1.4* | |
| Abbreviations: RDA, Recommended Dietary Allowance; AI, Adequate Intake; UL, Tolerable Upper Intake Level; µg, micrograms; mg, milligrams; g, grams; d, day; y, years; PUFA, polyunsaturated fatty acid | |||
References:
- Micronutrient Information Center in-depth article on Pregnancy and Lactation
- Nutrition: An Applied Approach, 4th edition. Janice Thompson and Melinda Manore. Chapter 15, Nutrition Through the Lifecycle: Pregnancy and the First Year of Life
- Present Knowledge in Nutrition, 10th edition. Chapter 39, Lindsay H. Allen, Maternal Nutrient Metabolism and Requirements in Pregnancy and Lactation
- Dietary Guidelines for Americans
- Dietary Reference Intake (DRI) reports
- Office on Women's Health, US Department of Health and Human Services
Nutrition Research
Essential Fatty Acids
What they do
General
- Essential fatty acids are a type of polyunsaturated fatty acid (PUFA) that cannot be synthesized in the body and must come from the diet.
- Essential fatty acids are structural components of every cell in the body and are converted to compounds that influence inflammation and immunity.
- There are two classes of essential fatty acids: omega-6 PUFA and omega-3 PUFA.
Pregnancy-specific
- The last trimester of pregnancy and first six months of postnatal life are critical periods for the accumulation of the long-chain omega-3 PUFA, docosahexaenoic acid (DHA), in the brain and retina of the baby.
What we know
- Most women of childbearing age and pregnant women in the US have low intakes of seafood and omega-3 PUFA.
- Higher intakes of long-chain omega-3 PUFA from fish and seafood during pregnancy are associated with improved developmental outcomes in offspring.
- Adequate omega-3 PUFA status in pregnant women protects against preterm birth (birth before 37 weeks’ gestation) and early preterm birth (birth before 34 weeks’ gestation), especially in those with low dietary DHA intake.
- Fetal tissue can form DHA from the omega-3 PUFA α-linolenic acid. If the maternal diet meets omega-3 PUFA (α-linolenic acid) and omega-6 PUFA (linoleic acid) requirements, supplementation with DHA provides no further benefit to the fetus.
- Supplementation with long-chain omega-3 PUFA during pregnancy modestly increases the length of gestation (1.6 days) and lowers the risk of preterm birth but does not reduce the risk of gestational diabetes mellitus, pregnancy-induced hypertension, or preeclampsia.
Highlight
- The potential benefits associated with obtaining long-chain omega-3 PUFA through moderate consumption of fish (one to two servings/week) during pregnancy outweigh any risks of contaminant exposure.
- The Dietary Guidelines for Americans recommend pregnant women consume 8 to 12 ounces/week of seafood, choosing options low in mercury.
- Fish with high levels of mercury (tilefish from the Gulf of Mexico, shark, swordfish, and king mackerel) should be avoided.
- Consumption of white (albacore) tuna should be limited to 6 ounces/week.
- See The US Food and Drug Administration for detailed advice on fish consumption.
For references and more information, see the sections on Visual and neurological development and Gestation and pregnancy in the Essential Fatty Acids article.

![]()
Biotin
What it is
General
- Biotin is a B-vitamin that helps make and break down glucose, fatty acids, and some amino acids.
Pregnancy-specific
- During pregnancy, biotin is needed for these same essential cellular activities, which are taking place at higher rates during fetal development.
What we know
- A substantial number of pregnant women (30 to 50 percent) have an increased urinary excretion of 3-hydroxyisovaleric acid (3-HIA), a marker of biotin status. It is not known whether this increase in urinary 3-HIA excretion is normal for pregnant women or indicative of low biotin intake relative to need.
- Although some animals are very sensitive to biotin deficiency during pregnancy, a link between biotin deficiency and adverse effects in the mother and the developing fetus has not been observed in humans.
- The recommended level of biotin intake (30 micrograms/day) is the same for pregnant and nonpregnant women (Table 2).
- Biotin is found in many foods, but the assessment of its dietary intake is hampered by the absence of biotin in nutrient composition databases. It is estimated that a varied diet in the US and Canada provides 30 to 60 micrograms of biotin per day.
For references and more information, see the section on Biotin in the Pregnancy and Lactation article.

![]()
Calcium
What it is
General
- Calcium is an essential mineral that is a structural component of bones and teeth, is required for proper nerve transmission and muscle contraction, and influences blood pressure.
Pregnancy-specific
- Approximately 250-350 milligrams (mg)/day of calcium is transferred from the mother to the fetus, primarily in the last trimester.
- Low-calcium intake during pregnancy may cause hormonal changes that lead to smooth muscle cell contraction, blood vessel narrowing, and the retention of sodium and fluid. These changes can contribute to the development of pregnancy-induced hypertension (PIH) and preeclampsia.
What we know
- Intestinal calcium absorption efficiency doubles during pregnancy, and the mineral can be temporarily mobilized from the skeleton to support fetal needs for calcium.
- Observational studies suggest an inverse relationship between dietary calcium intake and the occurrence of PIH. In other words, the lower the calcium intake, the higher the risk of developing PIH.
- Randomized controlled trials report that calcium supplementation during pregnancy (more than 1,000 mg/day) is associated with a 35 percent lower risk of high blood pressure and 55 percent lower risk of preeclampsia; the risk reduction for preeclampsia is even stronger for women considered to be at high risk for the condition (78 percent lower risk) and women with low dietary intake of calcium (64 percent lower risk).
- Although the RDA for calcium is the same for pregnant and nonpregnant women, calcium is considered a shortfall nutrient in the diet, and many women do not meet the recommended 1,000 mg/day.
- The World Health Organization (WHO) recommends daily calcium supplementation (1.5-2.0 g oral elemental calcium) to reduce the risk of preeclampsia for pregnant women in populations with low dietary calcium intake.
For references and more information, see the section on Calcium in the Pregnancy and Lactation article.
![]()
Choline
What it does
General
- Choline is an essential component of cell membranes, influences the production of several important neurotransmitters, and helps transport and metabolize fatty acids and cholesterol.
- Additionally, choline helps convert homocysteine to methionine, an amino acid used in countless essential cellular activities.
- Choline can be made by the body in small amounts but not enough to support health. Therefore, choline must also be obtained from dietary sources and is considered an essential nutrient.
Pregnancy-specific
- Choline is needed for embryonic and fetal brain development.
- Animal studies indicate that maternal intake of choline during pregnancy might affect intellectual abilities in the offspring.
What we know
- The mother delivers large amounts of choline to the fetus across the placental barrier, placing an increased demand on maternal stores of choline during pregnancy.
- Most pregnant individuals are not meeting the adequate intake (AI) for choline (450 mg/day); surveys estimate an average dietary intake ranging from 233 to 383 mg/day.
- Pregnant individuals are encouraged to consume choline-rich foods, such as eggs, meat, and seafood.
- Most pregnant individuals are not meeting the adequate intake (AI) for choline (450 mg/day); surveys estimate an average dietary intake ranging from 233 to 383 mg/day.
- The relationship between choline and the risk of neural tube defects is unclear at this time.
- There have been some reports that low dietary intake or low blood concentrations of choline are associated with a higher risk of NTDs; other reports have found no association.
- It is not known if supplementation with choline will lower the occurrence of NTDs.
For references and more information, see the section on Choline in the Pregnancy and Lactation article.
![]()
Chromium
What it does
General
- Chromium is a mineral that enhances the action of insulin.
Pregnancy-specific
- Chromium supplementation is being investigated for the control of blood glucose in type 2 diabetes mellitus; the role of chromium supplementation in gestational diabetes mellitus (GDM) is also under investigation.
What we know
- Observational studies report mixed results regarding serum chromium concentration and GDM.
- Two studies found no relationship; one study found that women with GDM have lower serum chromium concentration compared to pregnant women without GDM.
- Further complicating matters, it is not known if serum chromium concentration accurately reflects tissue chromium levels or chromium status during pregnancy.
- One small randomized controlled trial in 24 women with GDM found that supplementation with chromium picolinate significantly reduced fasting blood glucose and insulin levels. Importantly, insulin therapy was still required to normalize elevated blood glucose in this study population.
- More research is needed to determine whether chromium supplementation is useful in the treatment of GDM.
For references and more information, see the section on Chromium in the Pregnancy and Lactation article.
Folate (folic acid)
What it does
General
- Folate is a B-vitamin required for DNA synthesis and the formation of new cells.
- Additionally, the B-vitamins folate, vitamin B12, and vitamin B6 work together to convert homocysteine to methionine, an amino acid used in countless essential cellular activities.
- Folate is present naturally in food; folic acid is a synthetic form of folate that is found in supplements and fortified products. Although folic acid is better absorbed across the digestive tract, both forms enter the same biochemical pathway and are indistinguishable at the cellular level.
Pregnancy-specific
- The developing embryo and fetus require folate to form new cells, tissues, and organs.
- An especially sensitive event that relies on a sufficient amount of folate is the closure of the neural tube, the precursor to the brain and spinal cord. Closure of the neural tube occurs very early in pregnancy, by the sixth week of gestation, a time when many women do not realize they are pregnant.
What we know
- Lower blood folate concentrations are associated with a higher risk of neural tube defects (NTDs).
- Randomized controlled trials demonstrate that periconceptional supplementation with folic acid (i.e., beginning one month before conception until the end of the first trimester) dramatically reduces the occurrence of NTDs.
- In order to reduce the risk of NTDs, there is wide agreement that all persons capable of becoming pregnant take supplemental folic acid. The US Preventive Services Task Force recommends a daily supplement of 400 to 800 micrograms of folic acid for those planning or capable of pregnancy.
- Persons who have had a previous NTD-affected pregnancy or considered high-risk due to other factors (e.g., use of certain medications, family history) may be advised to consume up to 5,000 micrograms/day of folic acid when they are planning to become pregnant. This dosage should be prescribed and monitored by a healthcare provider.
- Throughout pregnancy, low blood folate concentrations may be associated with other adverse pregnancy outcomes. Elevated blood homocysteine, an indicator of low folate status, has been associated with an increased risk of preeclampsia, premature delivery, and low birth weight. For this reason, folic acid supplementation should continue throughout pregnancy.
For references and more information, see the section on Adverse pregnancy outcomes in the Folate article.
![]()
Iodine
What it does
General
- Iodine is a mineral that is a major structural component of thyroid hormones. Thyroid hormones regulate many key metabolic and enzymatic reactions that are essential for life.
Pregnancy-specific
- Iodine is needed for maternal thyroid hormone production.
- During pregnancy, thyroid hormone is needed for myelination of the central nervous system and is essential for normal brain development.
What we know
- Maternal iodine deficiency has been associated with increased incidence of miscarriage, stillbirth, and birth defects.
- Severe iodine deficiency during pregnancy can result in hypothyroidism and brain damage and mental deficiency in the offspring.
- Even mild forms of maternal iodine deficiency may have adverse effects on intellectual development and mental abilities in the offspring.
- The Recommended Dietary Allowance for iodine is significantly increased during pregnancy, from 150 to 220 micrograms/day.
- Universal salt iodization has helped to dramatically reduce iodine deficiency worldwide.
- Still, to ensure the higher requirement is met, the American Thyroid Association recommends that women take a multivitamin containing 150 micrograms of potassium iodide daily during preconception (ideally starting 3 months before a pregnancy), pregnancy, and lactation and advises all pregnant women to reach a daily intake of 250 micrograms of iodine — total combined from diet and supplements.
- The World Health Organization (WHO) and the United Nations International Children’s Emergency Fund (UNICEF) recommend iodine supplementation during pregnancy and lactation in regions where less than 20% of households have access to iodized salt.
- The American Thyroid Association advises against iodine intakes of 500 micrograms a day or more from iodine, potassium iodide, and kelp supplements during pregnancy and lactation.
For references and more information, see the section on Supplements in the Iodine article.

![]()
Iron
What it does
General
- Iron is required for the synthesis of hundreds of essential proteins, facilitates oxygen transport and storage, participates in energy production, and assists antioxidant enzymes.
- Dietary iron is found in two forms: heme and nonheme iron. Heme iron comes mainly from meat, poultry, and seafood. Nonheme iron is found in plants, dairy products, meat, fortified food.
Pregnancy-specific
- The developing fetus needs iron for the growth and development of all tissues and organs.
- The mother requires iron to meet the increased production of red blood cells that transport oxygen to the developing fetus; too little iron can lead to iron-deficiency anemia.
What we know
- The Recommended Dietary Allowance for iron is significantly increased during pregnancy, from 18 to 27 milligrams (mg)/day.
- Intestinal absorption of dietary iron increases during the second and third trimesters, yet many women still develop iron deficiency or iron-deficiency anemia during pregnancy.
- Severe iron deficiency during pregnancy has been associated with increased risk of maternal death, low-birth-weight infants, premature delivery, and perinatal mortality.
- In low-resource countries, where anemia is widespread and there is a high risk of anemia among pregnant women, daily iron supplementation during pregnancy reduces the risk of iron deficiency, anemia, preterm delivery, and low-birth-weight infants. Doses above 60 mg/day of elemental iron are associated with an increased risk of side effects.
- In high-resource countries, where there is a moderate prevalence of anemia among pregnant women, supplementation with iron improves maternal iron status and decreases the risk of anemia at term.
-
· Anemias are complex and can be caused by deficiencies in other micronutrients (folate, vitamin B12, vitamin A, and riboflavin) and non-nutritional causes (infection, inflammation, blood loss, and genetic disorders).
Highlight: Iron Supplements
- Most individuals will require iron supplements to meet the increased requirement during pregnancy.
- The Recommended Dietary Allowance during pregnancy is 27 mg iron/day, yet dietary surveys indicate that the average intake among pregnant women in the US is 15 mg/day.
- Health Canada recommends a supplement that has 16-20 mg of iron during pregnancy; the rest should come from diet.
- The US Centers for Disease Control and Prevention (CDC) recommend adequate dietary iron intake and iron supplementation (30 mg/day) beginning at the first prenatal visit.
- Reversible, gastrointestinal side effects (nausea, constipation, vomiting, and diarrhea) are associated with the use of high-dose (≥60 mg/day) iron supplements.
- Changing the dosing regimen or the form of iron supplement may reduce gastrointestinal side effects, for example:
- Intermittent, high-dose iron supplementation (one, two, or three times a week on non-consecutive days) may be a feasible alternative to daily supplementation among pregnant women who are not anemic and have adequate antenatal care.
- Oral ferrous bisglycinate, an amino acid iron chelate, has demonstrated higher bioavailability and fewer GI side effects compared to conventional iron supplements (i.e., ferrous iron salts such as ferrous sulfate, fumarate, gluconate, ascorbate, and glycine sulfate).
- Intermittent, high-dose iron supplementation (one, two, or three times a week on non-consecutive days) may be a feasible alternative to daily supplementation among pregnant women who are not anemic and have adequate antenatal care.
- Changing the dosing regimen or the form of iron supplement may reduce gastrointestinal side effects, for example:
- Vegetarians and vegans tend to have lower iron status compared to meat-eaters; iron absorption from dietary and supplemental sources can be enhanced by including vitamin C.
- In general, nonheme iron supplements are better absorbed on an empty stomach and with vitamin C.
- Take iron supplements separate (several hours apart) from single-dose calcium and zinc supplements.
- Do not take iron supplements with coffee, tea, bran, or milk.
For references and more information, see the section on Iron in the Pregnancy and Lactation article.
![]()
Magnesium
What it does
General
- Magnesium is an essential mineral that serves as a structural component of the skeleton; assists in hundreds of enzymatic reactions involved in the synthesis of energy, DNA, and proteins; and is required for proper nerve conduction and muscle contraction.
Pregnancy-specific
- Magnesium is needed for essential enzymatic reactions and the formation of new tissue (including bone) that takes place during embryonic and fetal development.
- Intravenous magnesium sulfate is included in the medical care of preeclampsia, eclampsia, and neuroprotection of premature infants.
What we know
- The RDA for magnesium is slightly increased during pregnancy, from 310 to 350 milligrams (mg)/day.
- Magnesium is considered a shortfall nutrient in the diet, meaning that magnesium is underconsumed by eating the typical American diet.
- Good sources of magnesium include green leafy vegetables, whole grains, and nuts.
- Regarding the medical management of certain pregnancy complications, intravenous magnesium sulfate causes blood vessel dilation in the brain and periphery and is used by physicians to prevent seizures that may occur in association with preeclampsia-eclampsia in late pregnancy or during labor.
- Intravenous magnesium sulfate has also been used by physicians to protect the brains of premature infants.
For references and more information, see the section on Pregnancy complications in the Magnesium article.
![]()
Riboflavin
What it does
General
- Riboflavin is a B-vitamin that helps convert food into useable energy and assists several metabolic and antioxidant enzymes.
Pregnancy-specific
- Riboflavin is needed to support the increased growth and energy utilization that occurs during pregnancy.
- While it is unclear what causes preeclampsia during pregnancy, riboflavin deficiency could compromise antioxidant enzyme activity, leading to oxidative stress and an increased risk of preeclampsia.
What we know
- In randomized controlled trials conducted in nonpregnant individuals, low-dose riboflavin supplementation (1.6 mg/day) may lower blood pressure in individuals with a genetic mutation in MTHFR, an enzyme involved in folate metabolism.
- Very few studies have investigated the link between riboflavin and preeclampsia.
- One observational study in pregnant women at high risk for preeclampsia found that those who were riboflavin deficient were 4.7 times more likely to develop preeclampsia than those who had adequate riboflavin nutritional status.
- One small randomized controlled trial in pregnant women at high risk for preeclampsia found that supplementation with 15 mg riboflavin daily did not prevent preeclampsia.
- The RDA for riboflavin is slightly increased during pregnancy, from 1.1 to 1.4 milligrams (mg)/day.
- Most plant and animal food contains riboflavin.
- Additionally, in the US and Canada, white flour has been enriched with riboflavin since the 1940s.
- Dietary surveys indicate that usual intake among Americans (≥4 years of age) is 2.2 mg/day.
For references and more information, see the section on Deficiency in the Riboflavin article.

![]()
Vitamin A
What it does
General
- Vitamin A is a fat-soluble vitamin that is essential for normal vision, reproduction, cell growth and development, and immune function.
- Preformed vitamin A (retinol) is found in animal organs and fortified products.
- Provitamin A carotenoids (α-carotene, β-carotene, and β-cryptoxanthin) are compounds found in yellow- and orange-colored fruit and vegetables that are converted to retinol by the liver.
Pregnancy-specific
- Vitamin A is involved in cellular events that regulate the formation of the vertebrae and spinal cord, vital organs (such as the heart and lungs), eyes, ears, and limbs. Severe vitamin A deficiency in animal models results in birth defects to these structures.
- Vitamin A deficiency impairs iron mobilization from stores, impairs the synthesis of hemoglobin, and may exacerbate iron-deficiency anemia.
- Because vitamin A is also required for normal functioning of the retina, dim-light vision, and color vision, vitamin A deficiency can lead to impaired dark adaptation (night blindness) and in severe cases, blindness.
What we know
- Vitamin A deficiency during pregnancy has been linked to impaired immunity, increased susceptibility to infection, increased risk of maternal death and disease, and night blindness.
- In regions of the world where vitamin A deficiency is a severe public health problem (mainly Africa and Southeast Asia), the World Health Organization (WHO) recommends vitamin A supplementation (up to 10,000 IU daily or 25,000 IU weekly) starting in the second or third trimester for the prevention of night blindness.
- In low-resource countries, co-supplementation with vitamin A and iron may be more effective in reducing iron-deficiency anemia than iron supplementation alone.
- Consumption of excess preformed vitamin A (retinol) during pregnancy can cause birth defects.
- The most critical period for damage appears to be during the first trimester, resulting in birth defects affecting the cardiovascular system, central nervous system, facial area, and thymus (an organ involved in immune cell production).
- Birth defects have not been observed at supplemental doses less than 3,000 micrograms (10,000 IU)/day of preformed vitamin A.
Highlight
- The slightly increased need for vitamin A during pregnancy (from 700 to 770 micrograms/day) can be met by consuming a varied and balanced diet and by consuming β-carotene, which is converted to vitamin A in the body and has not been associated with birth defects.
- In the US, vitamin A is considered a shortfall nutrient in the diet, and many women do not meet the recommended 700 micrograms/day.
- Because a number of foods in the US are fortified with preformed vitamin A, the Linus Pauling Institute recommends that pregnant individuals avoid multivitamin or prenatal supplements that contain more than 750 micrograms (2,500 IU) of preformed vitamin A (retinol).
For references and more information, see the section on Vitamin A in the Pregnancy and Lactation article.

![]()
Vitamin B6
What it does
General
- Vitamin B6 helps convert food into usable energy and assists in the formation of neurotransmitters, red blood cells, proteins, and DNA.
- Additionally, the B-vitamins folate, vitamin B12, and vitamin B6 work together to convert homocysteine to methionine, an amino acid used in countless essential cellular activities.
Pregnancy-specific
- Because a developing embryo and fetus have high rates of proliferation, they require vitamin B6 to form new cells, tissues, and organs.
- Vitamin B6 has been used since the 1940s to treat nausea during pregnancy.
What we know
- Short-term supplementation with high-dose vitamin B6 (10 mg/day) may help relieve nausea in pregnancy.
- The American and Canadian Colleges of Obstetrics and Gynecology recommend the use of a delayed-release formulation of pyridoxine hydrochloride (vitamin B6) plus doxylamine succinate (an antihistamine) as first-line therapy for nausea and vomiting during pregnancy. Such therapy should be conducted under the care of a qualified healthcare provider.
For references and more information, see the section on Nausea and vomiting during pregnancy in the Vitamin B6 article.
![]()
Vitamin B12
What it does
General
- Vitamin B12 helps convert food into usable energy, is required for proper nerve function, and assists in the formation of red blood cells, proteins, and DNA.
- Additionally, the B-vitamins folate, vitamin B12, and vitamin B6 work together to convert homocysteine to methionine, an amino acid used in countless essential cellular activities.
Pregnancy-specific
- Because a developing embryo and fetus have high rates of proliferation, they require vitamin B12 to form new cells, tissues, and organs.
What we know
- Absorption of vitamin B12 is more efficient during pregnancy.
- Inadequate dietary intake of vitamin B12 causes elevated homocysteine levels, which has been associated with adverse pregnancy outcomes, such as preeclampsia, premature delivery, low-birth weight and very low-birth-weight infants, and stillbirth.
- Low serum levels of vitamin B12 during pregnancy have been linked to an increased risk for neural tube defects (NTDs). However, the effect of vitamin B12 supplementation on the risk of NTDs has not yet been evaluated in randomized controlled trials.
- To ensure a daily intake of 6 to 30 micrograms of vitamin B12 in a form that is easily absorbed, the Linus Pauling Institute recommends that individuals who are planning a pregnancy take a daily multivitamin supplement or eat a breakfast cereal fortified with vitamin B12.
For references and more information, see the section on Vitamin B12 in the Pregnancy and Lactation article.
![]()
Vitamin C
What it does
General
- Vitamin C is a water-soluble vitamin that neutralizes a variety of reactive oxygen species (ROS) and recycles important cellular antioxidants.
- Vitamin C is also a cofactor in numerous enzymatic reactions involved in the making of collagen, L-carnitine, and several neurotransmitters, and in the regulation of gene expression.
- Vitamin C enhances the absorption of nonheme iron.
Pregnancy-specific
- Vitamin C is required to make collagen, a component of skin, blood vessels, tendons, and the organic matrix of bone.
- Oxidative stress has been implicated in the development of preeclampsia; thus, antioxidant vitamins (vitamin C and vitamin E) may be important in preventing the condition.
What we know
- Three pooled analyses of randomized controlled trials found no benefits of vitamin C supplementation, alone or in combination with other supplements, on pregnancy adverse events (preeclampsia, congenital malformations, stillbirth, perinatal death, preterm birth), with the exception of a reduced risk of placental abruption and a significant increase in gestational age at birth.
- Some research suggests that vitamin C supplementation during pregnancy may help reduce the risk of adverse pregnancy outcomes and respiratory illness in children born to women who continue to smoke throughout pregnancy, despite receiving counseling to quit.
For references and more information, see the section on Adverse pregnancy outcomes in the Vitamin C article.

![]()
Vitamin D
What it does
General
- Vitamin D is a fat-soluble vitamin that helps maintain calcium and phosphorus balance, promotes bone health, regulates immune function, and influences cell growth and development.
Pregnancy-specific
- Vitamin D is needed for the absorption of calcium and for the formation of new tissue (mainly bone) that takes place during embryonic and fetal development.
What we know
- Vitamin D insufficiency (defined by the National Academy of Medicine as serum 25-hydroxyvitamin D between 12 to 19 nanograms [ng]/milliliter [mL]) has been linked to an increased risk for a number of adverse outcomes in the mother and the infant.
- For the mother: gestational diabetes mellitus and preeclampsia.
- For the infant: preterm birth and low birth weight.
- Although other adverse outcomes have been examined, no significant relationships between vitamin D insufficiency and C-section, respiratory conditions, or allergies in children have been observed.
- The requirement for vitamin D (15 micrograms/day or 600 IU/day) is not increased during pregnancy, but vitamin D is considered a shortfall nutrient in the diet and low vitamin D status (less than 50 nmol/L [20 ng/mL]) is common in pregnant individuals.
| Country | Prevalence of Low Vitamin D Status in Pregnant or Lactating Women* |
|---|---|
| United States | 33% |
| Canada | 24% |
| United Kingdom | 35% |
| England | 31% |
| Spain | 20% |
| Netherlands | 44% |
| Germany | 77% |
| Turkey | 90% |
| Iran | 67% |
| Pakistan | 72% |
| Kuwait | 70-83% |
| India | 96% |
| China | 69% |
| Vietnam | 7% |
| Australia | 48% |
| *Palacios C and Gonzalez L. J Steroid Biochem Mol Biol. 2014 October; 144PA:138-45 | |
Highlight
- The RDA for pregnant individuals is 600 IU (15 micrograms) vitamin D/day, the same as for non-pregnant individuals.
- Vitamin D is notoriously difficult to obtain from food sources alone, and national surveys indicate that 94% of the US population is not meeting the dietary requirement for vitamin D.
- The Linus Pauling Institute recommends that generally healthy adults, including pregnant individuals, take 2,000 IU (50 micrograms) of supplemental vitamin D daily.
For references and more information, see the section on Adverse pregnancy outcomes in the Vitamin D article.
![]()
Vitamin E
What it does
General
- Vitamin E is a fat-soluble vitamin that functions as an antioxidant in lipid (fat) environments.
- Vitamin E is an important antioxidant nutrient in cell membranes, where it functions to protect cells from damage caused by reactive oxygen species (ROS).
Pregnancy-specific
- Oxidative stress has been implicated in the development of preeclampsia; thus, antioxidant vitamins (vitamin C and vitamin E) may be important in preventing the condition.
What we know
- Randomized controlled trials have not found combined supplementation of antioxidant vitamins (1,000 mg/day vitamin C plus 180 mg/day vitamin E [RRR-α-tocopherol]) to be effective in preventing preeclampsia.
For references and more information, see the section on Vitamin C and Vitamin E in the Pregnancy and Lactation article.

![]()
Vitamin K
What it does
General
- Vitamin K is a fat-soluble vitamin that assists in blood clotting and modifies certain proteins to a calcium-binding form.
- Naturally occurring vitamin K includes a number of different vitamin K compounds, classified as either vitamin K1 (phylloquinone) or vitamin K2 (menaquinones).
Pregnancy-specific
- When taken during pregnancy, a number of medications may increase the risk of vitamin K deficiency and hemorrhagic disease in the newborn. These medications include warfarin, rifampin, isoniazid, and anticonvulsants.
- Due to low placental transfer of vitamin K, a sterile gut, and immature liver, infants are born with low concentrations of vitamin K.
What we know
- Vitamin K deficiency bleeding (VKDB) develops in a small number of newborns who do not have enough vitamin K to form blood clots.
- Intramuscular (IM) injection of vitamin K to the newborn shortly after birth decreases the risk of VKDB.
- Oral administration of vitamin K to the newborn raises serum vitamin K concentration but is associated with an increased occurrence of late VKDB (bleeding that occurs 2 to 12 weeks after birth).
- The American Academy of Pediatrics and several international organizations recommend prophylactic IM injection of vitamin K1 within six hours of birth for the prevention of VKDB.
For references and more information, see the section on Vitamin K in the Pregnancy and Lactation article.

![]()
Zinc
What it does
General
- Zinc is an essential trace mineral that is required for the synthesis of hundreds of essential proteins, facilitates oxygen transport, and assists several antioxidant enzymes.
Pregnancy-specific
- Zinc is crucial for the formation, growth, and development of the cells and tissues of the developing fetus.
What we know
- The RDA for zinc is increased during pregnancy, from 8 to 11 mg/day (for ages 19 years and older).
- Poor nutritional status of zinc during pregnancy (variably assessed using hair, serum, red blood cell, or dietary indices) has been associated with a number of adverse outcomes, including preeclampsia, premature delivery, low-birth-weight newborns, and birth defects.
- Zinc supplementation in isolation is unlikely to benefit any pregnant individuals, whether they are from low- or high-resource settings.
- An emphasis on improving overall nutritional status rather than taking isolated zinc supplements is advised.
For references and more information, see the section on Pregnancy complications and adverse pregnancy outcomes in the Zinc article.
![]()
Alcoholic Beverages
What it does
General
- Alcoholic beverages contain ethanol and other ingredients with bioactive properties that may affect health.
- Moderate alcohol consumption is defined as no more than 2 drinks/day for men and no more than 1 drink/day for women.
Pregnancy-specific
- Ethanol is a teratogen, a substance that can cause abnormal development in the fetus.
- Alcohol in the mother’s blood readily crosses the placental barrier to the developing embryo or fetus.
What we know
- There is no known safe amount or safe time to drink alcohol during pregnancy.
- Alcohol consumption of any amount, especially during the first trimester, increases the risk of preterm birth and infants born small for gestational age.
- Moderate alcohol consumption during pregnancy has been associated with problems with memory, attention, learning, and behavior in the offspring.
- Regular heavy alcohol consumption (>4 drinks/day) and binge drinking (4 or more drinks per occasion) during pregnancy can lead to fetal alcohol syndrome, a group of lifelong physical, behavioral, and intellectual disabilities in the offspring.
For references and more information, see the section on Pregnancy in the Alcoholic Beverages article.
![]()
Coffee
What it does
General
- Coffee is a complex mixture of chemicals. In addition to caffeine, coffee contains several phytochemicals that can influence health.
Pregnancy-specific
- Caffeine crosses the placental barrier, and the fetus is exposed to caffeine via the umbilical cord and amniotic fluid.
- Caffeine is metabolized more slowly in pregnant individuals, with a half-life of about 15 hours in pregnant individuals compared to about five hours in nonpregnant women.
What we know
- Some, but not all, observational studies have associated high caffeine consumption (350-699 mg/day) with adverse effects during pregnancy, such as an increased risk of miscarriage and delivering a low-birth-weight baby.
- Individuals who are pregnant or planning to become pregnant should limit caffeine consumption to less than 200 milligrams (mg)/day.
| Food and Beverages | Caffeine Content (milligrams)* |
|---|---|
| Brewed coffee, 8 fluid ounces | 96 |
| Instant coffee, 1 teaspoon powder | 31 |
| Green tea, brewed from bag | 44 |
| Cola, 12 fluid ounces | 33 |
| Dark chocolate, 1 ounce | 24 |
| *Caffeine content can vary among commercial products. Search the USDA's FoodData Central for the caffeine content of a specific food or beverage. | |
Highlight
- Compounds in coffee can bind nonheme iron and inhibit its absorption.
- In general, dietary supplements should not be consumed with coffee.
For references and more information, see the section on Adverse pregnancy outcomes in the Coffee article.
Definitions
Anemia - a condition characterized by low concentration of hemoglobin
Animal experiment - a research experiment performed in a laboratory animal; many different animal species are studied in the laboratory, including terrestrial (land), aquatic (water), and microscopic animals.
Antioxidant - a compound that prevents or repairs the damage caused by reactive oxygen species
Antioxidant enzymes - enzymes which activities contribute to neutralizing atoms or molecules capable of damaging essential cell constituents
Conception - the point at which the egg is fertilized with the sperm
Eclampsia - progression of preeclampsia causing seizures and an increased risk of hemorrhage
Edema - significant fluid retention and swelling
Gestation - the period of development from conception until birth
Gestational diabetes mellitus (GDM) - high blood glucose during pregnancy
Hemoglobin - the oxygen-carrying component of red blood cells
Hypothyroidism - low concentration of thyroid hormone in the blood
Iron-deficiency anemia - a lack of iron in the body leads to decreased production of hemoglobin
Myelination - the accumulation of a fatty layer around nerve cells
Neural tube defects (NTDs) - a group of malformations that occur to the neural tube (the precursor to the brain and spinal cord) during embryonic development
Observational study - a human research study in which no experimental intervention or treatment is applied, and participants are simply observed over time
Oxidative stress - a situation in which the production of reactive oxygen species exceeds the ability of an organism to eliminate or neutralize them
Periconceptional - the period of time about one month before conception until the end of the first trimester
Placebo - a chemically inactive substance
Preeclampsia - abnormally high blood pressure accompanied by signs of organ damage (such as protein in the urine) and possibly edema
Pregnancy-induced hypertension - abnormally high blood pressure (>140/90 mm Hg) that develops after the twentieth week of pregnancy
Proliferation - an increase in the number or amount of something
Randomized controlled trial - a human research study in which participants are assigned by chance alone to receive either an experimental agent (the treatment group) or a placebo (the control group)
Reactive oxygen species (ROS) - highly unstable oxygen-containing compounds that react easily with nearby cellular structures, potentially causing damage
Authors and Reviewers
Originally written in March 2016 by:
Giana Angelo, Ph.D.
Linus Pauling Institute
Oregon State University
Updated in August 2025 by:
Giana Angelo, Ph.D.
Linus Pauling Institute
Oregon State University
Reviewed in August 2025 by:
Crystal Karakochuk, Ph.D.
Associate Professor, Human Nutrition
Canada Research Chair Tier 2 in Micronutrients and Human Health
The University of British Columbia
The 2025 update was underwritten, in part, by a grant from Balchem Corporation.
Copyright 2016-2026 Linus Pauling Institute
Figure Alternative Text
Figure. Essential fatty acids and dietary sources
The figure shows two vertical pathways of essential fatty acid metabolism, with dietary sources of the main fatty acids listed.
Omega-6 pathway: At the top, linoleic acid (LA; dietary sources include vegetable oils and safflower oil) is metabolized to γ-linolenic acid (GLA), then to dihomo-γ-linolenic acid (DGLA), and finally to arachidonic acid (AA; dietary sources include meat, poultry, and eggs).
Omega-3 pathway: At the top, α-linolenic acid (ALA; dietary sources include green leafy vegetables; flax and chia seeds; and canola, walnut, and soybean oils) is metabolized to stearidonic acid (SDA), then to eicosatetraenoic acid (ETA), and then to eicosapentaenoic acid (EPA; dietary sources include oily fish, algae oil, and krill oil). EPA is further metabolized to docosapentaenoic acid (DPA), and ultimately to docosahexaenoic acid (DHA; dietary sources include oily fish, krill oil, and algae oil).
Disclaimer
The Linus Pauling Institute's Micronutrient Information Center provides scientific information on the health aspects of dietary factors and supplements, food, and beverages for the general public. The information is made available with the understanding that the author and publisher are not providing medical, psychological, or nutritional counseling services on this site. The information should not be used in place of a consultation with a competent health care or nutrition professional.
The information on dietary factors and supplements, food, and beverages contained on this website does not cover all possible uses, actions, precautions, side effects, and interactions. It is not intended as nutritional or medical advice for individual problems. Liability for individual actions or omissions based upon the contents of this site is expressly disclaimed.
You may not copy, modify, distribute, display, transmit, perform, publish or sell any of the copyrightable material on this website. You may hyperlink to this website but must include the following statement:
"This link leads to a website provided by the Linus Pauling Institute at Oregon State University. [Your name] is not affiliated or endorsed by the Linus Pauling Institute or Oregon State University."